
JCRM , 1(2), 25; doi:10.65381/jcrm.2026.01020025
Review
Lentigines Removal Using Lee-Chan Radiofrequency Ablation-Intense Pulsed Light Technique: Case Series and Literature Review
Kar Wai Alvin Lee 1,* ,
Kwin Wah Lisa Chan 1
and
Cheuk Hung Lee 1
,
Kwin Wah Lisa Chan 1
and
Cheuk Hung Lee 1
,
Kwin Wah Lisa Chan 1
and
Cheuk Hung Lee 1
1
Everkeen Medical Centre, Hong Kong
*
Correspondence: alvin429@yahoo.com
Academic Editor:
Siu Chung Patrick Leung
Received: 7 June 2026 / Accepted: 7 June 2026 / Published: 11 June 2026
Abstract
:Background: Lentigines, particularly solar lentigines, are common benign pigmented lesions arising predominantly on chronically sun-exposed skin. Although medically benign, they frequently generate significant cosmetic concern and may impair self-image, especially when numerous, enlarging, recurrent, or distributed over highly visible facial and acral sites. Established treatment options include topical depigmenting agents, cryotherapy, chemical peels, pigment-specific lasers, and intense pulsed light (IPL). However, selected patients desire more immediate lesion removal than can be achieved with topical therapy alone, while ablative approaches may produce post-inflammatory hyperpigmentation (PIH), particularly in Fitzpatrick skin types III–VI. Aim: Radiofrequency ablation (RFA) allows rapid focal lesion destruction with hemostasis and precision, whereas IPL is an established modality for treating residual dyschromia and broader photodamage. This case series and literature review evaluates the efficacy and safety of the Lee-Chan radiofrequency ablation-intense pulsed light technique for lentigines removal and subsequent pigment optimization. Methods: Three patients with extensive benign pigmented facial lesions were treated using the Lee-Chan staged protocol. The updated series comprised one patient with big lentigine and two patients with extensive predominant solar lentigines, one of whom also had background dyschromia with melasma. Because of the extensive facial involvement, radiofrequency surgical treatment was performed in two sessions separated by 4 weeks, followed by intense pulsed light (IPL) after re-epithelialization to reduce post-procedural hyperpigmentation, residual pigmentation, and generalized photodamage. Clinical outcomes included lesion clearance, textural improvement, pigment reduction, skin quality, cosmetic blending, downtime, tolerability, and patient-reported satisfaction. Results: Across the updated three cases, radiofrequency treatment achieved effective removal of the targeted benign pigmented lesions with excellent procedural control and no major complications. Subsequent IPL contributed to reduction of residual dyschromia and post-procedural pigmentation while also improving overall skin texture, pore prominence, tone uniformity, and perceived facial rejuvenation. At final follow-up, the patients showed high cosmetic acceptability, no hypertrophic scarring, and marked improvement in the treated areas, including enhanced skin glow, softening of fine wrinkles, and visible tightening in selected regions. Conclusions: The Lee-Chan RFA-IPL technique appears to be a practical and cosmetically advantageous staged approach for selected patients with extensive benign pigmented facial lesions, including solar lentigines and related seborrheic keratotic changes. Radiofrequency treatment provides immediate focal lesion removal, whereas IPL serves as a complementary modality for minimizing residual pigmentation, improving photodamaged skin, and optimizing the final aesthetic result. The updated case series further supports the value of combining lesion-directed ablation with subsequent field-based light therapy in patients concerned about scarring, hyperpigmentation, and overall facial rejuvenation.
Keywords:
lentigo; radiofrequency ablation; intense pulsed light therapy; hyperpigmentation; skin aging; wound healing1. Introduction
Lentigines are sharply circumscribed pigmented macules or slightly elevated lesions characterized clinically by persistent brown to dark-brown coloration that does not fade seasonally [1]. Among the various subtypes, solar lentigines are the most frequently encountered in everyday dermatologic and aesthetic practice [2]. They arise predominantly on chronically sun-exposed areas including the face, dorsal hands, forearms, upper chest, and shoulders, and their prevalence increases with cumulative ultraviolet exposure and advancing age [3]. Although benign, solar lentigines are highly visible markers of photoaging and are a common reason for cosmetic consultation [4].
From a pathobiologic perspective, solar lentigines represent a chronic photodamage-associated alteration involving increased melanocytic activity, increased melanin deposition, and epidermal architectural change [5]. Histopathologic studies have demonstrated increased epidermal melanin, increased melanocyte density compared with adjacent photodamaged skin, and variable epidermal hyperplasia or flattening [6]. Interestingly, facial solar lentigines may not always show the classic elongated rete ridge pattern often described in nonfacial lentigines, emphasizing the importance of clinicopathologic correlation when evaluating pigmented lesions on photoaged facial skin [7].
The clinical burden of lentigines should not be underestimated. While asymptomatic in most patients, they frequently produce psychosocial distress by conveying an aged, unhealthy, or cosmetically neglected appearance [8]. Patients with extensive facial lentigines often report reduced self-confidence, greater reliance on camouflage cosmetics, and frustration with slowly acting topical regimens [9]. In Asian populations and other skin-of-color groups, concern is magnified by the coexistence of uneven tone, background tanning, melasma tendency, and a greater risk of treatment-induced dyschromia [10].
A broad therapeutic armamentarium exists for lentigines management. Topical agents such as hydroquinone, mequinol/tretinoin, retinoids, cysteamine, azelaic acid, and combination pigment-correcting formulations may improve selected lesions, but response is gradual and often incomplete [4]. Cryotherapy can be effective for discrete lesions but may cause blistering, hypopigmentation, prolonged erythema, and textural change [11,12]. Chemical peels can improve diffuse photodamage but carry irritation-related risk, especially in reactive skin [13]. Laser and light-based technologies, including Q-switched lasers, picosecond lasers, pulsed dye laser in selected contexts, and IPL, are frequently used with good efficacy, yet treatment response varies by lesion depth, phototype, and device selection [14].
Among current modalities, IPL occupies a particularly important role because it can target melanin while simultaneously improving broader signs of photodamage such as mottled pigmentation, telangiectasia, and mild textural irregularity [15]. Recent reviews suggest that IPL is an effective therapy for solar lentigines, with good-to-excellent responses reported in many studies and generally acceptable safety when appropriate filters and fluences are selected. Nonetheless, IPL alone may be less immediately gratifying for patients who desire same-day removal of sharply demarcated or darker focal lesions, and multiple treatment sessions are often required [16].
Radiofrequency ablation offers a different therapeutic logic. By delivering high-frequency alternating current, RFA generates localized thermal destruction of targeted tissue with simultaneous coagulation, thereby permitting focal lesion removal with excellent hemostasis and relative procedural efficiency [17]. In benign cutaneous lesions, RF technology has been reported to be safe and effective across a range of epidermal and superficial dermal lesions, including lentigo among other nonvascular lesions [18]. Its advantages include accessibility, rapid learning curve, precise contact treatment, and the ability to debulk or remove individual lesions in a single visit. However, because it is an ablative modality, it can provoke inflammation-associated dyschromia, particularly PIH, in patients with darker skin types or in those receiving treatment over cosmetically prominent sites.
PIH remains one of the most clinically important adverse sequelae after cutaneous injury or energy-based treatment [19]. It results from inflammation-induced stimulation of melanogenesis, increased melanin transfer to keratinocytes, and, in some cases, pigment incontinence with dermal melanophages [20]. Patients with Fitzpatrick skin types IV–VI are especially susceptible, though PIH can occur in any phototype. Even when the primary lesion is successfully removed, residual brown discoloration may leave the patient dissatisfied and may undermine the perceived success of the procedure.
This creates the rationale for the Lee-Chan radiofrequency ablation-intense pulsed light technique. In this combined strategy, focal RFA is used first to remove the discrete benign lentigines, especially lesions that are darker, more numerous, cosmetically conspicuous, or refractory to previous topical treatment. After complete wound healing, IPL is introduced to address post-procedural pigmentation, residual chromatic irregularity, and the surrounding field of photodamaged skin [21]. Conceptually, this allows the clinician to unite the immediate precision of ablative lesion removal with the color-correcting and rejuvenative capacity of light-based therapy.
Despite the biologic plausibility of this combined approach, formal literature specifically evaluating sequential RFA followed by IPL for lentigines remains limited. Most published work has focused either on IPL monotherapy for solar lentigines or on RFA as a treatment for benign cutaneous lesions more generally. Thus, there is a need for descriptive clinical reporting on how a staged combination protocol performs in real practice, especially in Asian patients and others vulnerable to pigmentary sequelae.
The objectives of this case series and literature review are therefore fourfold. First, to evaluate the practical efficacy of focal RFA for immediate lentigines removal. Second, to document the frequency and characteristics of residual pigmentation or PIH after ablation. Third, to assess the contribution of subsequent IPL in improving dyschromia and overall cosmetic blending. Fourth, to review the relevant literature regarding lentigines biology, differential diagnosis, current treatment modalities, the mechanism and advantages of RFA, and the role of IPL in pigment correction and field rejuvenation.
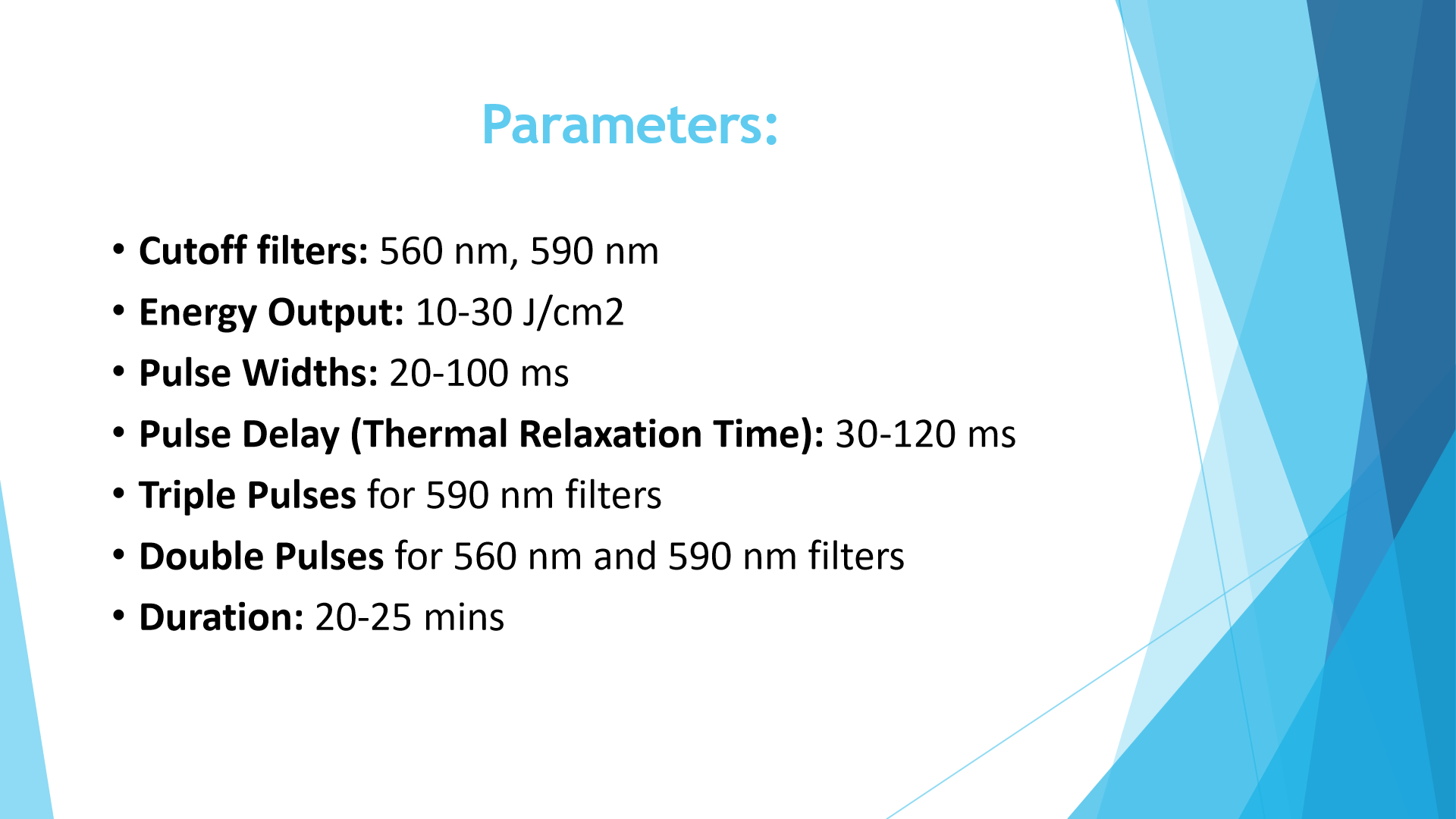
Three individuals with clinically identified lentigines with different severities are presented in this case series. Following radiofrequency ablation with the Ellman Surgitron 4.0 Dual RF 120 IEC system (Figure 1), all patients were monitored for the development of post-inflammatory hyperpigmentation. Intense pulsed light therapy utilizing the Lumenis M22 platform (Figure 2) was given to patients who developed clinically significant post-inflammatory hyperpigmentation in accordance with a defined protocol (Figure 3).
Figure 1.
Ellman Surgitron 4.0 Dual RF 120 IEC.
Figure 2.
Lumenis M22 Intense Pulsed Light machine.

Figure 3.
Intense Pulsed Light treatment parameters.
In the following sections, we present three representative patients treated using this integrated protocol. Each case is organized in the same structure: history, physical examination, treatment, and post-treatment follow-up. The purpose is not only to report outcomes but also to illustrate patient selection, procedural sequencing, and practical issues encountered during daily aesthetic and dermatologic practice.
2. Case 1: Extensive Left Facial Lentigines with Associated Photoaging Changes
2.1. Case 1 History
Mr. M., a 52-year-old man, presented with a dark patch over the left side of the face that had been present for more than 10 years. He reported that the lesion had progressively enlarged over the preceding 2–3 years and was occasionally associated with an itching sensation.
He had previously sought medical advice, but was warned about the possibility of scar formation and an even higher chance of darker post-inflammatory hyperpigmentation after treatment. These concerns discouraged him from pursuing earlier intervention.
His past health history was notable for cigarette smoking for 20 years and the use of antihyperlipidaemic medication. After assessment, he was counselled and offered radiofrequency surgical treatment followed by intense pulsed light (IPL) therapy to optimize pigment clearance and cosmetic outcome.
2.2. Case 1 Physical Examination
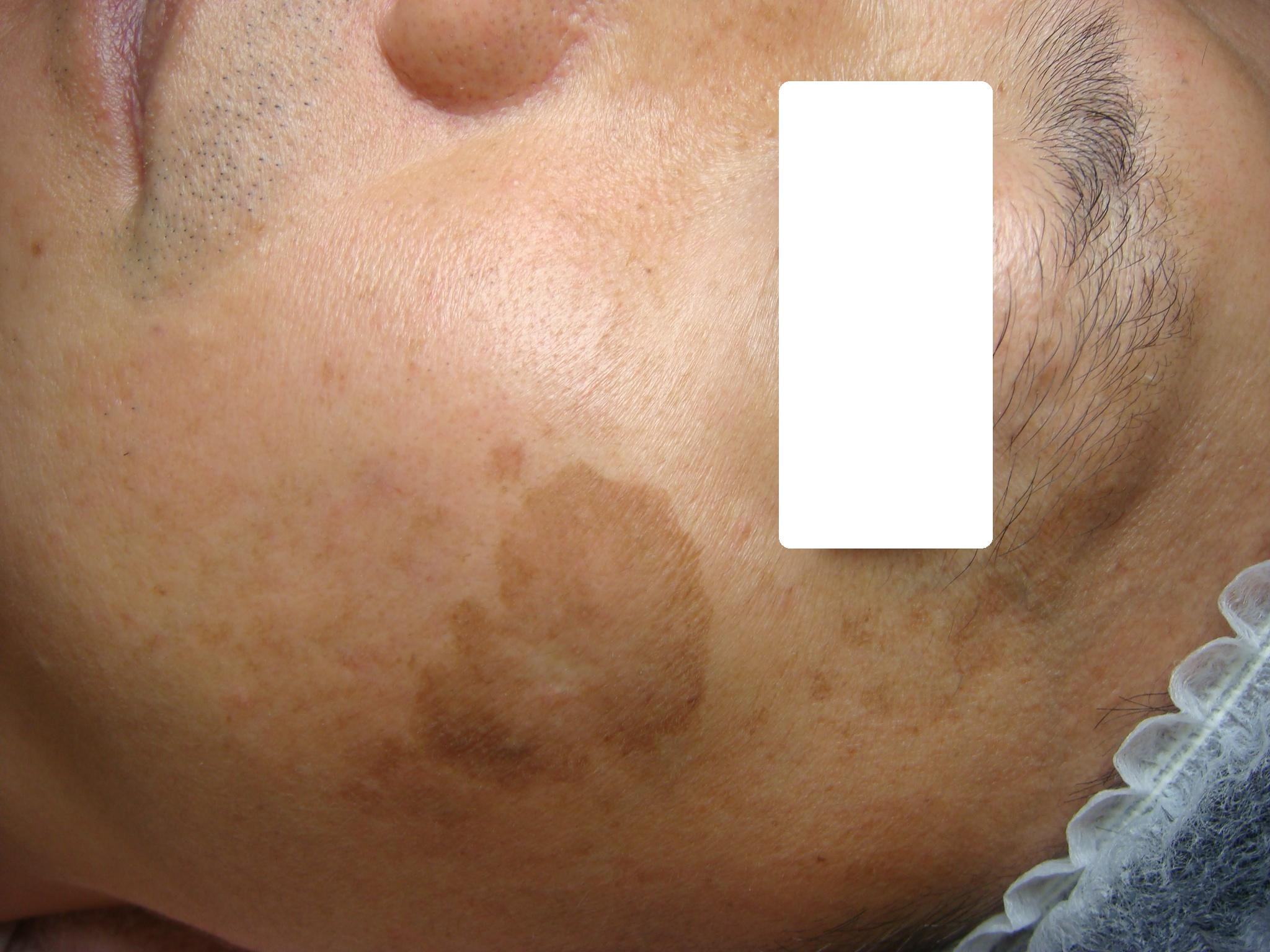
Physical examination revealed a large dark-brown patch with a rough surface over the left side of the face, measuring approximately 7 × 4.5 cm, clinically consistent with lentigine. Several smaller light-brown lentiginous patches were present surrounding the main lesion, with additional smaller lesions noted over the upper eyelid and eyebrow region.
The facial skin showed a relatively darker complexion with distinct fine wrinkles in the infraorbital region, particularly below the eyebag. The overall appearance suggested concurrent photodamage and early facial aging changes (Figure 4).
Figure 4.
Left face of Case 1 before radiofrequency ablation treatment, showing large patch of lentigine.
Figure 4.
Left face of Case 1 before radiofrequency ablation treatment, showing large patch of lentigine.
2.3. Case 1 Treatment
In view of the size and cosmetic prominence of the lesion, radiofrequency surgical treatment was recommended as the primary lesion-directed procedure. This was followed by IPL as an adjunctive treatment after healing, with the aim of reducing residual pigmentation, improving skin tone uniformity, and enhancing the overall cosmetic result.
The patient was counselled regarding the risks and benefits of treatment, including the possibility of pigmentary alteration, the importance of post-procedural care, and the role of IPL in improving both pigmentation and background skin quality.
2.4. Case 1 Post-Treatment Follow-Up
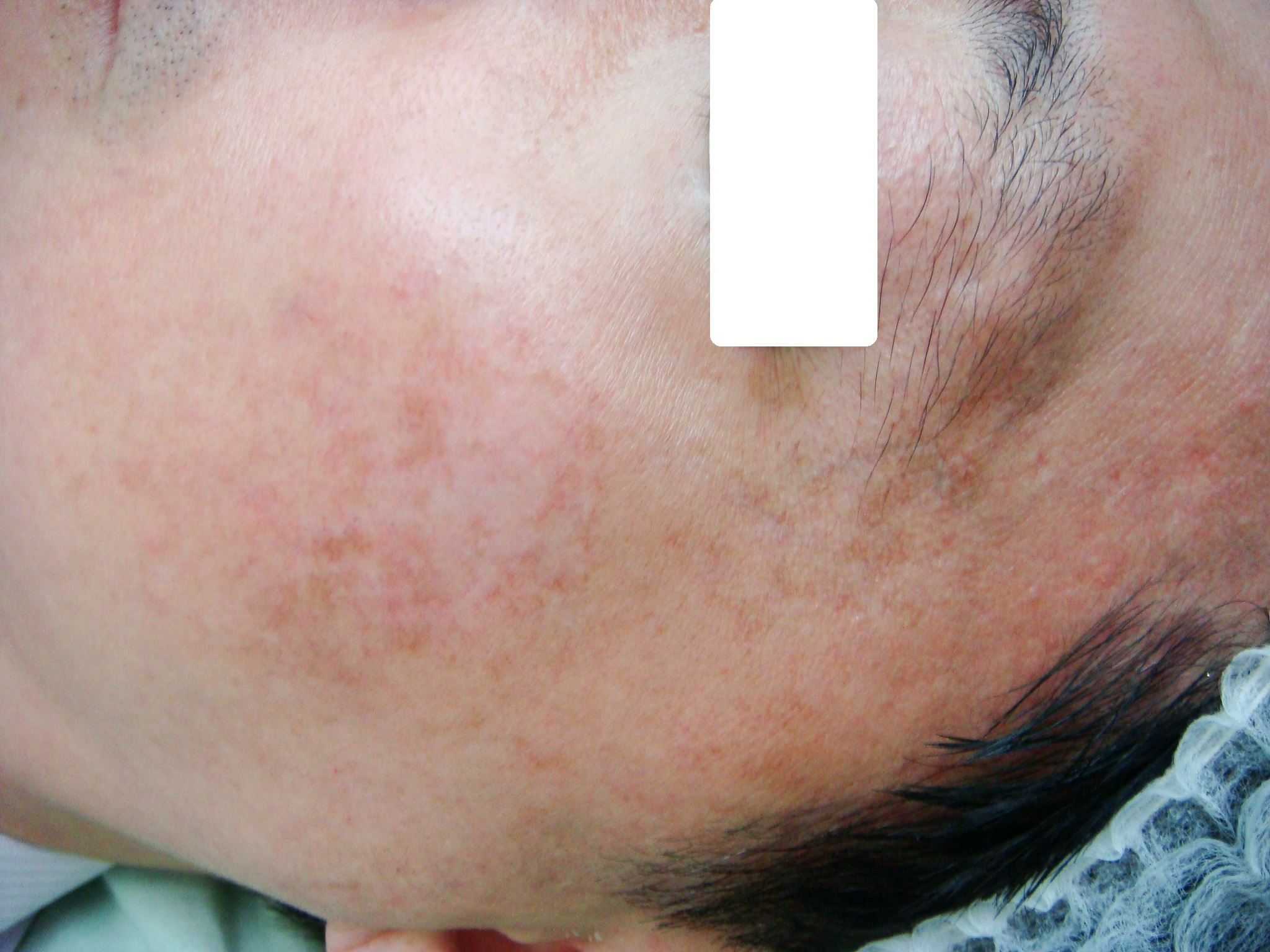
At follow-up, the large lentiginous patch had almost completely cleared. There was also marked improvement in overall facial skin texture, with the treated skin appearing brighter and more rejuvenated.
In addition, the fine wrinkles below the eyebag were noticeably diminished. The skin rejuvenation effect was considered to be largely attributable to the adjunctive IPL treatment, which contributed not only to pigment optimization but also to improvement in texture and overall appearance (Figure 5).
Figure 5.
Left face of Case 1 after Lee-Chan radiofrequency ablation intense pulsed light technique management.
Figure 5.
Left face of Case 1 after Lee-Chan radiofrequency ablation intense pulsed light technique management.
3. Case 2: Extensive Facial Solar Lentigines in a Patient Concerned About Pain, Scarring, and Hyperpigmentation
3.1. Case 2 History
Ms. T., a 47-year-old woman, presented with numerous dark and grey facial patches that had been present for more than 15 years and had increased in both number and size during the preceding 5 years. She was especially distressed by the facial visibility of the lesions and reported being teased by colleagues because of the multiple darker patches.
She had avoided treatment because she was very afraid of painful procedures and was also worried about possible scarring and even worse hyperpigmentation after intervention. She did not routinely use formal sun-protection measures apart from wearing hats during outdoor activities.
Her past health history was unremarkable apart from the use of contraceptive pills. Given the extensive facial involvement, she was counselled and offered radiofrequency surgical treatment in 2 sessions separated by 4 weeks, with subsequent IPL to reduce the risk of scarring and post-inflammatory hyperpigmentation.
3.2. Case 2 Physical Examination
Examination revealed numerous flat dull-grey and brown patches of solar lentigines distributed over both sides of the face, ranging from approximately 2 mm to 1.5 cm in size. Darker patches were also present at the lateral aspect of the left eyebrow and upper eyelid.
A few associated seborrheic keratotic lesions were noted on the forehead, lip, and right lateral face. The skin showed mild laxity with a somewhat wavy facial outline, and fine wrinkles were prominent in the lower eyebag regions.
Pretreatment photography documented the widespread distribution of the facial lentigines and the accompanying signs of early facial laxity and lower eyelid wrinkling before initiation of staged therapy (Figure 6).
Figure 6.
Front view of Case 2 before treatment, showing multiple lentigines over bilateral cheeks and frontal area.
Figure 6.
Front view of Case 2 before treatment, showing multiple lentigines over bilateral cheeks and frontal area.

3.3. Case 2 Treatment
Because of the extensive whole-face involvement, staged radiofrequency surgical treatment was planned in 2 sessions separated by 4 weeks. This approach was selected to allow controlled removal of the widespread lesions while limiting the chance of excessive inflammatory response in a cosmetically sensitive area.
Following the radiofrequency sessions, IPL was administered as an adjunctive treatment to reduce the risk of scarring and hyperpigmentation and to improve the surrounding photodamaged facial skin. The patient was counselled about careful post-procedure skin care and the importance of ongoing sun protection.
The treatment strategy was accepted because it balanced her wish for visible lesion removal with her strong concerns about pain, post-treatment marks, and overall cosmetic recovery.
3.4. Case 2 Post-Treatment Follow-Up
The patient completed the staged protocol uneventfully. At follow-up, all solar lentigine lesions had been removed, with obvious improvement in overall skin texture, pore prominence, and facial glow.
Fine wrinkles in the lower eyebag regions were also improved substantially. In addition, tightening of the whole face was evident, with a smoother and more curved facial outline replacing the baseline wavy contour.
The result was cosmetically gratifying to the patient and addressed both pigmentary concerns and broader signs of facial aging without clinically significant scarring during the documented follow-up (Figure 7).
Figure 7.
Front view of Case 2 after Lee-Chan radiofrequency ablation intense pulsed light technique management.
Figure 7.
Front view of Case 2 after Lee-Chan radiofrequency ablation intense pulsed light technique management.

4. Case 3: Facial Solar Lentigines with Background Dyschromia, Melasma, and Associated Seborrheic Keratotic Lesions
4.1. Case 3 History
Ms. L., a 62-year-old woman, presented with a darker facial complexion together with multiple darker papules and patches over both sides of the face and the temple regions for approximately 12–13 years. She reported that the lesions had increased in number and size more recently.
She was a regular morning trail walker but seldom applied sunscreen because she found sun-protection cream too sticky. She sought treatment because her daughter was going to marry and she wished to improve her appearance for the wedding events.
Her past health history included antihypertensive and cardiac medications. She was counselled regarding the small but important possibility of scarring and hyperpigmentation and the need for strict sun-protective measures during outdoor activity after treatment. Because of the extensive facial involvement, she was offered radiofrequency surgical treatment in 2 sessions separated by 4 weeks, followed by IPL.
4.2. Case 3 Physical Examination
Examination showed several flat dull-grey and brown patches of solar lentigines, approximately 2 mm to 1.3 cm in size, over both lateral sides of the face. These lesions were superimposed on a background of generalized dyschromic discoloration with melasma.
A few seborrheic keratotic lesions were also present over both temporal regions, the right lower eyebag, and the mid-forehead. The skin pores were widened and coarse, and fine wrinkles were prominent in the lower eyebag regions.
Telangiectasia was visible at the corners of the mouth. Pretreatment photography was obtained to document the mixed pigmentary and textural changes before staged therapy (Figure 8).
Figure 8.
Front view of Case 3 before treatment, showing multiple large lentigines.

4.3. Case 3 Treatment
Because of the extensive facial involvement and mixed lesion pattern, radiofrequency surgical treatment was planned in 2 sessions separated by 4 weeks. The treatment targeted the clinically evident lentigines and associated raised benign pigmented lesions while aiming to preserve smooth healing over the surrounding facial skin.
After the ablative stage, IPL was used as an adjunctive modality to reduce the risk of post-inflammatory hyperpigmentation and to address residual pigmentation and overall photodamaged skin quality. The patient was reminded that continuous sun protection would be essential for maintaining the result.
The staged Lee-Chan approach was selected because it offered both immediate lesion-directed treatment and broader field improvement in tone, texture, and vascular irregularity.
4.4. Case 3 Post-Treatment Follow-Up
The patient completed the planned treatment course with satisfactory healing. At follow-up, all solar lentigine lesions had been removed, and the skin texture had improved markedly, producing a shiny and glistening appearance, especially over the forehead, together with minimization of pore size.
Fine wrinkles in the lower eyebag regions were also improved substantially after treatment. In addition, amelioration of the perioral telangiectasia was noted, contributing to a more even and rejuvenated appearance.
Overall, the cosmetic outcome was highly favorable, with improvement not only in the focal lentigines but also in the broader dyschromia and associated signs of facial photoaging during the documented follow-up period (Figure 9).
Figure 9.
Front view of Case 3 after Lee-Chan radiofrequency ablation intense pulsed light technique management.
Figure 9.
Front view of Case 3 after Lee-Chan radiofrequency ablation intense pulsed light technique management.

5. Discussion
5.1. Epidemiology and Pathogenesis of Lentigines
Solar lentigines are among the most common pigmentary manifestations of chronic photodamage. They occur predominantly in middle-aged and older adults, especially on the face, dorsal hands, forearms, chest, and upper back. In lighter skin types, prevalence increases markedly with age, but solar lentigines are also highly relevant in Asian populations, where they frequently present on the face and contribute significantly to perceived facial aging. Their development is closely related to chronic ultraviolet radiation exposure, episodic sunburn, and cumulative environmental photodamage [11].
Histologically, solar lentigines represent more than a simple “excess melanin spot.” Quantitative and descriptive studies have shown increased epidermal melanin and increased melanocyte numbers relative to adjacent photodamaged skin, together with variable epidermal architectural change. Facial lesions may demonstrate either epidermal hyperplasia with elongated pigmented rete ridges or a relatively flattened epidermis with basal melanosis and more severe solar elastosis. These findings help explain the clinical heterogeneity of lentigines and likely contribute to variable responsiveness across treatment modalities [22].
The photobiology of lentigines also has practical therapeutic implications. Lesions are not uniform in depth, epidermal architecture, or adjacent field change. A patient may therefore exhibit a mixture of sharply demarcated darker lesions suitable for focal destruction and broader low-contrast pigmentation better suited to light-based field therapy [23]. This observation forms an important conceptual basis for combining RFA and IPL rather than relying on a single modality for all lesions.
5.2. Clinical Presentation and Differential Diagnosis
Clinically, solar lentigines are well-demarcated tan, brown, or dark-brown macules, occasionally slightly raised, typically asymptomatic, and situated on chronically sun-exposed skin [5]. They may appear as isolated lesions or as part of a more generalized photoaging pattern. In aesthetic practice, patients often present not because of symptoms but because of cumulative cosmetic burden, lesion prominence in photography, or increasing contrast between treated facial skin and untreated hands or temples.
However, not every pigmented macule on photoaged skin is a benign lentigo. The differential diagnosis includes ephelides, macular seborrheic keratosis, pigmented actinic keratosis, post-inflammatory hyperpigmentation, lichen planus-like keratosis, melasma fragments, flat melanocytic nevus [24], and most importantly lentigo maligna [25]. Dermoscopy is therefore essential, and biopsy should be performed for any lesion with asymmetry, irregular gray pigmentation, evolving borders, follicular obliteration, nodularity, ulceration, or diagnostic uncertainty [26]. Any manuscript or clinical protocol describing lentigines removal should emphasize that lesion selection and exclusion of malignancy are prerequisites, not optional steps.
5.2.1. Treatment Modalities for Lentigines
Therapeutic choices for lentigines include topical therapies, destructive procedures, and energy-based devices. Topical agents are useful for diffuse dyschromia and for patients preferring low-downtime care, but they require weeks to months of adherence and may be limited by irritation, rebound pigmentation, or incomplete lesion-specific clearing. Cryotherapy is inexpensive and commonly used for discrete lesions, but its risk profile can be problematic in darker or reactive skin, with blistering, erythema, textural alteration, and hypopigmentation not infrequently encountered [11].
Lasers and IPL have become central to modern treatment algorithms. A recent systematic review of clinical trials concluded that laser- and light-based modalities are among the most effective options for solar lentigines [27]. IPL in particular showed favorable efficacy, with reported good-to-excellent improvement in a substantial proportion of facial and hand lesions and a generally acceptable safety profile. A targeted short-wavelength IPL protocol in Japanese patients with Fitzpatrick III-V skin showed significant improvement after a single treatment and high satisfaction, with only minor transient adverse events [28]. These data reinforce the role of IPL as a valuable modality for benign pigmentary lesions and field photorejuvenation.
Yet even effective monotherapy has limitations. IPL may require multiple sessions and may not instantly remove the darkest or most sharply delineated lesions to the degree some patients desire. Laser modalities may be highly effective but can be costlier, less accessible, and still carry PIH risk in susceptible patients. In daily practice, a hybrid strategy may therefore better match patient expectations in selected cases.
5.2.2. Mechanisms and Advantages of Radiofrequency Ablation
Radiofrequency technology delivers high-frequency alternating current that produces heat within tissue through resistance, resulting in controlled cutting, vaporization, and coagulation [29]. In benign cutaneous lesions, RF devices have been reported to offer efficient tissue destruction, precision, and excellent hemostasis, with good-to-excellent outcomes in most nonvascular lesions and high patient satisfaction. For clinicians already experienced with radiosurgery, RFA is often quicker and more accessible than pigment-specific laser platforms [30].
For lentigines, the advantages of focal RFA are primarily practical rather than theoretical elegance. It can remove the darkest or most cosmetically dominant lesions during a single visit, creating an immediate sense of progress that many patients value. It also permits lesion-by-lesion customization and is relatively independent of optical target competition from adjacent diffuse pigmentation. In addition, the inherent coagulative effect of RF allows a clean and controlled operative field.
However, RFA is not a universal first-line treatment for every lentigo. Its utility is greatest when the clinician has carefully selected clearly benign lesions and when the patient specifically desires prompt focal removal. Because it is ablative, it predictably induces a wound-healing response and therefore carries risk of PIH and textural change. Over-treatment, deep passes, or poor aftercare can worsen outcome. Thus, the role of RFA in lentigines should be framed as selective and technically disciplined [31,32].
5.3. The Lee-Chan RFA-IPL Technique: Integrated Approach
The central innovation of this technique lies not in a novel device, but in sequencing. RFA and IPL are used for different purposes at different stages of the same problem. RFA provides immediate focal removal of the lesions that most visibly trouble the patient. IPL is then introduced only after re-epithelialization to refine pigment, reduce PIH, and improve the surrounding field. This avoids using IPL as a rescue for an incompletely healed wound while still leveraging its pigment-corrective value.
From a workflow standpoint, the technique is straightforward. Step 1 is rigorous selection of benign lesions with exclusion of suspicious pigmented lesions. Step 2 is conservative focal RFA with meticulous attention to depth and thermal spread. Step 3 is structured wound care and strict photoprotection. Step 4 is delayed IPL after epithelial recovery. Step 5 is serial follow-up for recurrence, pigment evolution, and patient satisfaction. This technique was also applied in treating scars [33], other sources of PIH [33,34], viral warts [35]. IPL alone can also be used in treating severe erythematotelangiectatic rosacea [36], vitiligo [37] and acne fulminans [38].
In the present case series, the combined approach appeared especially useful in patients who wanted immediate visible lesion removal but were also highly concerned about cosmetic blending. The technique seemed adaptable across facial and hand sites, although settings and aggressiveness required tailoring to location and phototype.
5.3.1. Clinical Considerations and Patient Selection
Ideal candidates for the Lee-Chan technique are patients with clinically typical benign lentigines who desire rapid focal lesion removal, have failed or declined topical therapy, and are willing to adhere to sun protection and staged follow-up. It may be particularly appealing in patients with a small-to-moderate number of cosmetically dominant lesions superimposed on generalized photodamage.
Caution is necessary in patients with very dark phototypes, active inflammatory dermatoses, recent tanning, poor adherence likelihood, or a strong history of severe PIH [39]. In such patients, a more conservative hybrid approach may be preferable, treating only the darkest lesions with RFA and leaving less conspicuous or diffuse pigmentation for IPL or topical therapy alone. Suspicious pigmented lesions should never be ablated without diagnostic certainty.
5.3.2. Complications and Management
Potential complications of focal RFA include pain, prolonged crusting, infection, textural irregularity, scarring, hypopigmentation, hyperpigmentation, and incomplete lesion removal [40]. Among these, PIH is likely the most common and most relevant cosmetic issue. Practical management includes conservative initial settings, superficial passes, gentle debridement of carbonized debris rather than repeated deep passes, strict wound care, and intensive UV avoidance [41].
Potential complications of IPL include transient erythema, discomfort, swelling, blistering, and paradoxical pigmentary change. These can be minimized by phototype-appropriate settings, cooling, avoidance of tanning, and careful timing after complete healing of ablated sites. The clinician must remember that IPL is being used here as a refinement phase, not as an excuse to overtreat during the initial ablation phase [42].
5.3.3. Recurrence Rates and Long-Term Outcomes
Because lentigines arise in the setting of chronic photodamage, long-term follow-up must distinguish between true recurrence of a treated lesion and development of new lentigines in adjacent sun-damaged skin. RFA may remove the index lesion completely, yet continued ultraviolet exposure can produce future lesions nearby. This is one reason why adjunctive IPL and long-term photoprotection may improve the overall perceived durability of treatment [43,44].
In our staged framework, recurrence should be assessed at both lesion and field levels. Lesion-level recurrence refers to reappearance at the exact previously treated site. Field-level progression refers to emergence of new pigmentary lesions in the same photodamaged zone. Counseling patients on this distinction can improve satisfaction and reduce misunderstanding regarding the realistic goals of treatment.
5.3.4. Cost-Effectiveness Considerations
From a practical perspective, RFA is often more accessible than pigment-specific lasers and may be more cost-effective for removing a limited number of discrete cosmetically dominant lesions. Meanwhile, IPL offers broader photorejuvenation value by treating residual pigment and the surrounding field in the same session. For selected patients, the combined approach may therefore provide a favorable balance between immediate focal improvement and broader cosmetic enhancement [38].
That said, cost-effectiveness depends heavily on lesion burden. A patient with only diffuse light lentigines and no need for immediate focal removal might be better managed with IPL or laser alone. Conversely, a patient with a few very dark lesions might achieve satisfactory results with RFA alone if pigmentary risk is low. The Lee-Chan technique appears most rational in the “middle group”: patients with discrete dominant lesions plus broader dyschromia.
5.3.5. Future Directions and Research Needs
Several research questions remain open. Prospective studies should compare RFA alone, IPL alone, and staged RFA-IPL treatment using standardized lesion photography, blinded assessment, melanin index measurements, and patient-reported outcome instruments. Future work should also stratify results by phototype, lesion location, and lesion morphology, because these factors likely influence both efficacy and PIH risk.
Additional investigation into prophylactic anti-PIH strategies is also warranted, particularly in Asian and darker phototype populations. Whether adjunctive topical corticosteroids, tranexamic acid, or pigment-suppressive regimens improve outcomes after lentigines ablation deserves systematic evaluation. Finally, histologic and dermoscopic correlation studies may help identify which lentigines are most suitable for focal ablative removal versus light-based therapy alone.
6. Conclusions
Lentigines are common benign pigmentary lesions that frequently generate disproportionate cosmetic and psychosocial burden, especially when numerous, facially distributed, or superimposed on diffuse photodamage. Modern treatment options are diverse, but each has limitations related to speed, cost, accessibility, downtime, or risk of dyschromia.
The present manuscript proposes the Lee-Chan radiofrequency ablation-intense pulsed light technique as a staged, practical, and cosmetically oriented strategy for selected benign lentigines. In this approach, focal RFA is used for immediate lesion removal with precision and hemostasis, while delayed IPL addresses residual pigmentation, PIH, and broader color irregularity. The combined sequencing is particularly attractive in patients who desire rapid visible change but remain highly concerned about post-procedural pigmentary sequelae.
Based on the current case series framework and existing literature, this integrated technique appears promising, especially for cosmetically significant lesions in Asian patients and other populations at increased risk of PIH. Nevertheless, careful patient selection, exclusion of malignant mimics, conservative treatment depth, disciplined aftercare, and rigorous photoprotection remain essential. Larger prospective studies are needed before definitive comparative conclusions can be drawn.
Author Contributions
All authors have reviewed and approved the article for submission. Conceptualization, K.W.A.L., K.W.L.C. and C.H.L. Writing-Originial Draft Preparation, K.W.A.L., K.W.L.C. and C.H.L. Writing-Review and Editing, K.W.A.L., K.W.L.C. and C.H.L. Visualization, K.W.A.L., K.W.L.C. and C.H.L. Supervision, C.H.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data are available by contacting the corresponding author.
Conflicts of Interest
I acknowledge that I have considered the conflict of interest statement included in the Author Guidelines. I hearby certify that, to the best of my knowledge, no aspect of my current personal or professional situation might reasonably be expected to significantly affect my views on the subject I am presenting.
References
- Han, A.; Bressack, M.; Wilson, J.L. Disorders of pigmentation. Prim. Care Clin. Off. Pract. 2025, 52(3), 623–650. [Google Scholar] [CrossRef]
- Ortonne, J.P.; Pandya, A.G.; Lui, H.; Hexsel, D. Treatment of solar lentigines. J. Am. Acad. Dermatol. 2006, 54(5), S262–S271. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Morita, A.; Seité, S.; Haarmann-Stemmann, T.; Grether-Beck, S.; Krutmann, J. Environment-induced lentigines: Formation of solar lentigines beyond ultraviolet radiation. Exp. Dermatol. 2015, 24(6), 407–411. [Google Scholar] [CrossRef]
- Mardani, G.; Nasiri, M.J.; Namazi, N.; Farshchian, M.; Abdollahimajd, F. Treatment of solar lentigines: A systematic review of clinical trials. J. Cosmet. Dermatol. 2025, 24(4), e70133. [Google Scholar] [CrossRef]
- Manganelli, M.; Stabile, G.; Scharf, C.; Podo Brunetti, A.; Paolino, G.; Giuffrida, R.; Bigotto, G.D.; Damiano, G.; Mercuri, S.R.; Sallustio, F.; Mangano, E. Skin photodamage and melanomagenesis: A comprehensive review. Cancers 2025, 17(11), 1784. [Google Scholar] [CrossRef]
- Gómez-Martín, I.; Moreno, S.; Andrades-López, E.; Hernández-Muñoz, I.; Gallardo, F.; Barranco, C.; Pujol, R.M.; Segura, S. Histopathologic and immunohistochemical correlates of confocal descriptors in pigmented facial macules on photodamaged skin. JAMA Dermatol. 2017, 153(8), 771–780. [Google Scholar] [CrossRef]
- Shin, J.; Park, J.Y.; Kim, S.J.; Kang, H.Y. Characteristics of keratinocytes in facial solar lentigo with flattened rete ridges: Comparison with melasma. Clin. Exp. Dermatol. 2015, 40(5), 489–494. [Google Scholar] [CrossRef] [PubMed]
- Carniciu, S.; Hafi, B.; Gkini, M.A.; Tzellos, T.; Jafferany, M.; Stamu-O’Brien, C. Secondary psychiatric disorders and the skin. Dermatol. Rev. 2023, 4(4), 162–171. [Google Scholar] [CrossRef]
- Kornhaber, R.; Visentin, D.; Thapa, D.K.; West, S.; McKittrick, A.; Haik, J.; Cleary, M. Cosmetic camouflage improves quality of life among patients with skin disfigurement: A systematic review. Body Image 2018, 27, 98–108. [Google Scholar] [CrossRef]
- Lim, H.W.; Zhang, C.; Taylor, M.; Dlova, N.C.; Conceição, K.; Jablonski, N.; Gupta, N.; Wangari-Olivero, J.; Alexis, A. International expert consensus on knowledge gaps in care for dermatologic disorders in skin of color. Int. J. Dermatol. 2026, 65(1), 41–56. [Google Scholar] [CrossRef] [PubMed]
- Mukovozov, I.; Roesler, J.; Kashetsky, N.; Gregory, A. Treatment of lentigines: A systematic review. Dermatol. Surg. 2023, 49, 17–24. [Google Scholar] [CrossRef]
- Stem, R.S.; Dover, J.S.; Levin, J.A.; Arndt, K.A. Laser therapy versus cryotherapy of lentigines: A comparative trial. J. Am. Acad. Dermatol. 1994, 30(6), 985–987. [Google Scholar] [CrossRef]
- Cotellessa, C.; Peris, K.; Onorati, M.T.; Fargnoli, M.C.; Chimenti, S. The use of chemical peelings in the treatment of different cutaneous hyperpigmentations. Dermatol. Surg. 1999, 25(6), 450–454. [Google Scholar] [CrossRef]
- Ho, S.G.; Chan, N.P.; Yeung, C.K.; Shek, S.Y.; Kono, T.; Chan, H.H. A retrospective analysis of the management of freckles and lentigines using four different pigment lasers on Asian skin. J. Cosmet. Laser Ther. 2012, 14(2), 74–80. [Google Scholar] [CrossRef]
- Friedmann, D.P.; Peterson, J.D. Efficacy and safety of intense pulsed light with a KTP filter for the treatment of solar lentigines. Lasers Surg. Med. 2019, 51(6), 500–508. [Google Scholar] [CrossRef]
- Kawada, A.; Shiraishi, H.; Asai, M.; Kameyama, H.; Sangen, Y.; Aragane, Y.; Tezuka, T. Clinical improvement of solar lentigines and ephelides with an intense pulsed light source. Dermatol. Surg. 2002, 28(6), 504–508. [Google Scholar] [PubMed]
- Keum, H.; Cevik, E.; Kim, J.; Demirlenk, Y.M.; Atar, D.; Saini, G.; Sheth, R.A.; Deipolyi, A.R.; Oklu, R. Tissue ablation: Applications and perspectives. Adv. Mater. 2024, 36(32), 2310856. [Google Scholar] [CrossRef]
- Atiyeh, B.S.; Dibo, S.A. Nonsurgical nonablative treatment of aging skin: Radiofrequency technologies between aggressive marketing and evidence-based efficacy. Aesthetic Plast. Surg. 2009, 33(3), 283–294. [Google Scholar] [CrossRef]
- Kashetsky, N.; Feschuk, A.; Pratt, M.E. Post-inflammatory hyperpigmentation: A systematic review of treatment outcomes. J. Eur. Acad. Dermatol. Venereol. 2024, 38(3), 470–479. [Google Scholar] [CrossRef] [PubMed]
- Lamel, S.A.; Rahvar, M.; Maibach, H.I. Postinflammatory hyperpigmentation secondary to external insult: An overview of the quantitative analysis of pigmentation. Cutan. Ocul. Toxicol. 2013, 32(1), 67–71. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, D.; Kostaki, D.; Crisman, G. Quick Guide to Dermoscopy in Laser and IPL Treatments; Springer International Publishing: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Andersen, W.K.; Labadie, R.R.; Bhawan, J. Histopathology of solar lentigines of the face: A quantitative study. J. Am. Acad. Dermatol. 1997, 36(3), 444–447. [Google Scholar] [CrossRef]
- Feng, H.; Kauvar, A.N. Lentigines and dyschromia. In Evidence-Based Procedural Dermatology; Springer International Publishing: Cham, Switzerland, 2019; pp. 917–931. [Google Scholar]
- Zhu, W.Y.; Li, L.; Zhang, R.Z.; Peng, S.W.; Wang, H.W.; Tan, C.; Xu, L.; Pan, M.; Tian, Z.H.; Zhao, X.D.; Xing, Y.L. Pigmentary disorder. In Atlas of Skin Disorders: Challenging Presentations of Common to Rare Conditions; Springer: Singapore, 2018; pp. 243–280. [Google Scholar]
- Kasprzak, J.M.; Xu, Y.G. Diagnosis and management of lentigo maligna: A review. Drugs Context 2015, 4, 212281. [Google Scholar] [CrossRef]
- Krueger, L.; Saizan, A.; Stein, J.A.; Elbuluk, N. Dermoscopy of acquired pigmentary disorders: A comprehensive review. Int. J. Dermatol. 2022, 61(1), 7–19. [Google Scholar] [CrossRef]
- Putri, P.M.; Savitri, I.D. The Analysis Study of Efficacy and Effectiveness of Laser and Light Therapy for The Treatment of Cutaneous Disorders of Hyperpigmentation: A Comprehensive Systematic Review. Int. J. Med. Sci. Health Res. 2024, 2(4), 49–62. [Google Scholar] [CrossRef]
- Tanaka, Y.; Tsunemi, Y.; Kawashima, M. Objective assessment of intensive targeted treatment for solar lentigines using intense pulsed light with wavelengths between 500 and 635 nm. Lasers Surg. Med. 2016, 48(1), 30–35. [Google Scholar] [CrossRef]
- Görgü, M.; Gökkaya, A.; Kizilkan, J.; Karanfil, E.; Dogan, A. Radiofrequency: Review of literature. Turk. J. Plast. Surg. 2019, 27(2), 62–72. [Google Scholar] [CrossRef] [PubMed]
- Dawson, E.; Willey, A.; Lee, K. Adverse events associated with nonablative cutaneous laser, radiofrequency, and light-based devices. In Seminars in Cutaneous Medicine and Surgery; WB Saunders Co.: Philadelphia, PA, USA, 2007; Volume 26, pp. 15–21. [Google Scholar]
- Sachdeva, S.; Dogra, A. Radiofrequency ablation in dermatology. Indian J. Dermatol. 2007, 52(3), 134–137. [Google Scholar] [CrossRef]
- Fernandez-Guarino, M.; Naharro-Rodriguez, J.; Bacci, S. Aberrances of the wound healing process: A review. Cosmetics 2024, 11(6), 209. [Google Scholar] [CrossRef]
- Chan, L.K.W.; Lee, K.W.A.; Hung, L.C.; Lam, P.K.W.; Wan, J.; Vitale, M.; Huang, P.P.; Yi, K. Treating hypertrophic scar, post-inflammatory hyperpigmentation, and post-inflammatory hypopigmentation with intense pulsed light. Skin Res. Technol. 2024, 30, e13823. [Google Scholar] [CrossRef]
- Lee, C.H.; Lee, K.W.A.; Chan, K.W. Experience of using intense pulsed light safely and effectively, with cases sharing of treating postinflammatory hyperpigmentation with different origins. J. Cosmet. Med. 2024, 8, 66–71. [Google Scholar] [CrossRef]
- Lee, K.W.A.; Chan, K.W.L.; Lee, C.H.; Wong, T.H.S. Viral Wart Removal Using Lee-Chan Radiofrequency Ablation-Intense Pulsed Light Technique: Case Series and Literature Review. J. Cosmet. Regen. Med. 2026, 1, 5. [Google Scholar]
- Hung, L.C.; Alvin, L.K.W.; Wah, C.K. Treatment of severe erythematotelangiectatic rosacea with intense pulsed light: A case report. J. Cosmet. Med. 2023, 7, 38–41. [Google Scholar] [CrossRef]
- Lee, C.H.; Lee, K.W.A.; Chan, K.W. Case report: Treating vitiligo with intense pulsed light. J. Cosmet. Med. 2023, 7, 42–44. [Google Scholar] [CrossRef]
- Lee, C.H.; Lee, K.W.A.; Chan, K.W.; Lam, K.W.P. Treatment of acne fulminans with intense pulsed light: A case report. J. Cosmet. Med. 2022, 6, 99–102. [Google Scholar] [CrossRef]
- Maghfour, J.; Olayinka, J.; Hamzavi, I.H.; Mohammad, T.F. A focused review on the pathophysiology of post-inflammatory hyperpigmentation. Pigment. Cell Melanoma Res. 2022, 35(3), 320–327. [Google Scholar] [CrossRef]
- Tanzi, E.L.; Alster, T.S. Complications of Ablative and Nonablative. In Complications in Cutaneous Surgery; Elsevier: Amsterdam, The Netherlands, 2010; p. 167. [Google Scholar]
- Olutoye, O.O.; Eriksson, E.; Menchaca, A.D.; Kirsner, R.S.; Tanaka, R.; Schultz, G.; Weir, D.; Wagner, T.L.; Fabia, R.B.; Naik-Mathuria, B.; Liu, P.Y. Management of acute wounds—Expert panel consensus statement. Adv. Wound Care 2024, 13(11), 553–583. [Google Scholar] [CrossRef] [PubMed]
- Stangl, S.; Hadshiew, I.; Kimmig, W. Side effects and complications using intense pulsed light (IPL) sources. Med. Laser Appl. 2008, 23(1), 15–20. [Google Scholar] [CrossRef]
- Stege, H. Light protection: Before and after IPL, laser, and PDT treatments. In Energy for the Skin: Effects and Side-Effects of Lasers, Flash Lamps and Other Sources of Energy; Springer International Publishing: Cham, Switzerland, 2022; pp. 401–406. [Google Scholar]
- Sakamoto, F.H.; Avram, M.M.; Anderson, R.R. Lasers and Other Energy-Based Technologies-Principles and Skin Interactions. In Dermatology, 4th ed.; Elsevier: Philadelphia, PA, USA, 2018; pp. 2354–2363. [Google Scholar]
© 2026 copyright by the authors. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).